Xin chào các bạn,
Tôi là một bác sỹ ngoại tim mạch đang thực hiện một đề tài liên quan đến AI và DL. Cũng là lần đầu tiên tiếp cận với AI vs DL. Đề ứng dụng đo đường kính và thể tích động mạch chủ. Phần mềm ARVA của một công ty AI Pháp Incepto medical đã thực hiện đo động mạch chủ bụng, lần này tôi tiến hành đo trên động mạch chủ ngực. Mặc dù công việc của tôi chỉ là dùng phần mềm đo. Nhưng tôi mong muốn hiểu thêm về cách hoạt động của AI vs DL trong phần mềm này. Tôi hy vọng nhận được nhiều góp ý và giải thích cơ chế AI vs DL của ứng dụng này cho một ngừoi ngoài chuyên ngành như tôi. Xin trân trọng cảm ơn.
Thân ái.
Một nghiên cứu ứng dụng trong Y khoa đo trên động mạch chủ bụng
Objective: The aim of this study was to evaluate an automatic, deep learning based method (Augmented Radiology for Vascular Aneurysm [ARVA]), to detect and assess maximum aortic diameter, providing cross sectional outer to outer aortic wall measurements.
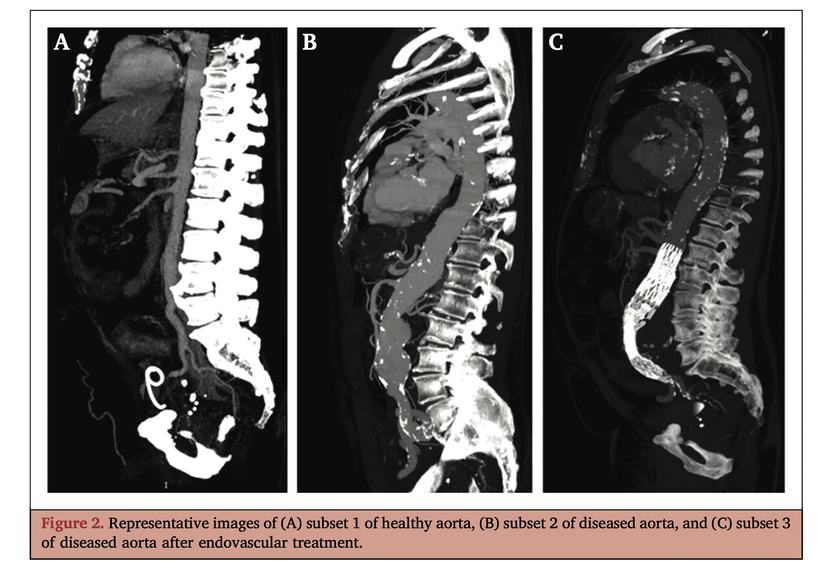
Methods: Accurate external aortic wall diameter measurement is performed along the entire aorta, from the ascending aorta to the iliac bifurcations, on both pre- and post-operative contrast enhanced computed tomography angiography (CTA) scans. A training database of 489 CTAs was used to train a pipeline of neural networks for automatic external aortic wall measurements. Another database of 62 CTAs, including controls, aneurysmal aortas, and aortic dissections scanned before and/or after endovascular or open repair, was used for validation. The measurements of maximum external aortic wall diameter made by ARVA were compared with those of seven clinicians on this validation dataset.
Results: The median absolute difference with respect to expert’s measurements ranged from 1 mm to 2 mm among all annotators, while ARVA reported a median absolute difference of 1.2 mm.
Conclusion: The performance of the automatic maximum aortic diameter method falls within the interannotator variability, making it a potentially reliable solution for assisting clinical practice.
Automatic pipeline
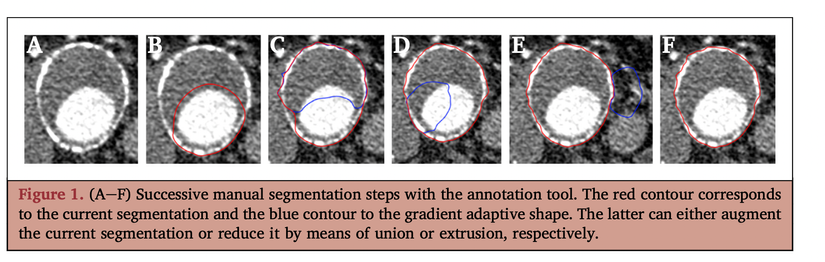
Pipeline steps. The proposed algorithms pipeline leverages neural network learning abilities and aims to reproduce diameter measurements performed by clinicians. It is composed of five successive steps.
Step 1: localisation. The aorta is, in general, a relatively small structure (in width) in the body, compared with other organs. To maintain enough resolution during segmentation without requiring excessive use of memory, first a fully convolutional network is used to regress the bounding box coordinates of the aorta. All volumes in the training set are resampled to a fixed size of (160, 160, 160). The architecture used is the following: four convolution blocks, each con- taining three convolutional layers, and ending with a global average pooling layer, resulting in six values corresponding to the coordinates of the upper left and the lower right corners of the aortic bounding box. The number of kernels used in the 12 resulting convolutional layers is (16, 16, 16); (32, 32, 32); (64, 64, 64); (128, 128, 6). All kernel sizes are fixed to (3, 3, 3). Each convolution layer is followed by a ReLU activation and a batch normalisation step. Maxpooling (factor 2) is applied after each convolution block, and final global average pooling is followed by a ReLU activation to output the final result. Optimisation is performed using an Adam optimiser, an L1 regression loss, and a learning rate starting at 1e-5 and being divided by two every 20 epochs. Optimisation was done over a total of 60 epochs. The training database was augmented using random trans- lations and zooms limited to 10 mm and a factor variation of 0.1, respectively.
Step 2: segmentation. Following the localisation step, the predicted bounding box is used to perform a crop of the box containing the aorta at full resolution. This crop is further resampled to a fixed size of (160, 160, 160). The full seg- mentation of the aorta (lumen and thrombus) is performed using a V-Net architecture,5 with a symmetrical structure. Both its descending and ascending branches are composed of three convolution blocks, each containing three con- volutional layers. The number of kernels used in the nine resulting convolutional layers is (16, 16, 16); (32, 32, 32); (64, 64, 64). All kernel sizes are fixed to (3, 3, 3). Between convolutional layers and convolution blocks, the same layers as in the localisation network are used. The final activation function is a sigmoid to ensure output values in the range [0,1]. To train this network we use a combination of a Dice coefficient loss (one over the Dice coefficient) and a cross entropy loss. Optimisation is done using an Adam optimiser with a starting learning rate of 1e-4 and divided by two every 15 epochs. A total of 50 epochs was enough for convergence.
Step 3: segmentation refinement. This step uses the full resolution volume and the segmentation mask obtained in the previous step. It aims at correcting errors made by the V-Net generating by its inferior working resolution. A fixed number of iterations (10 in the current version) of the fuzzy region competition algorithm was performed.6
Step 4: centreline. Using a minimal path algorithm,7 the centrelines of the main branches of the aorta (main trunk and iliac arteries) are computed based on both lumen and thrombus. This step is subtle, and crucial, as all subsequent
measurements depend on it. Centrelines should be well positioned and smooth.
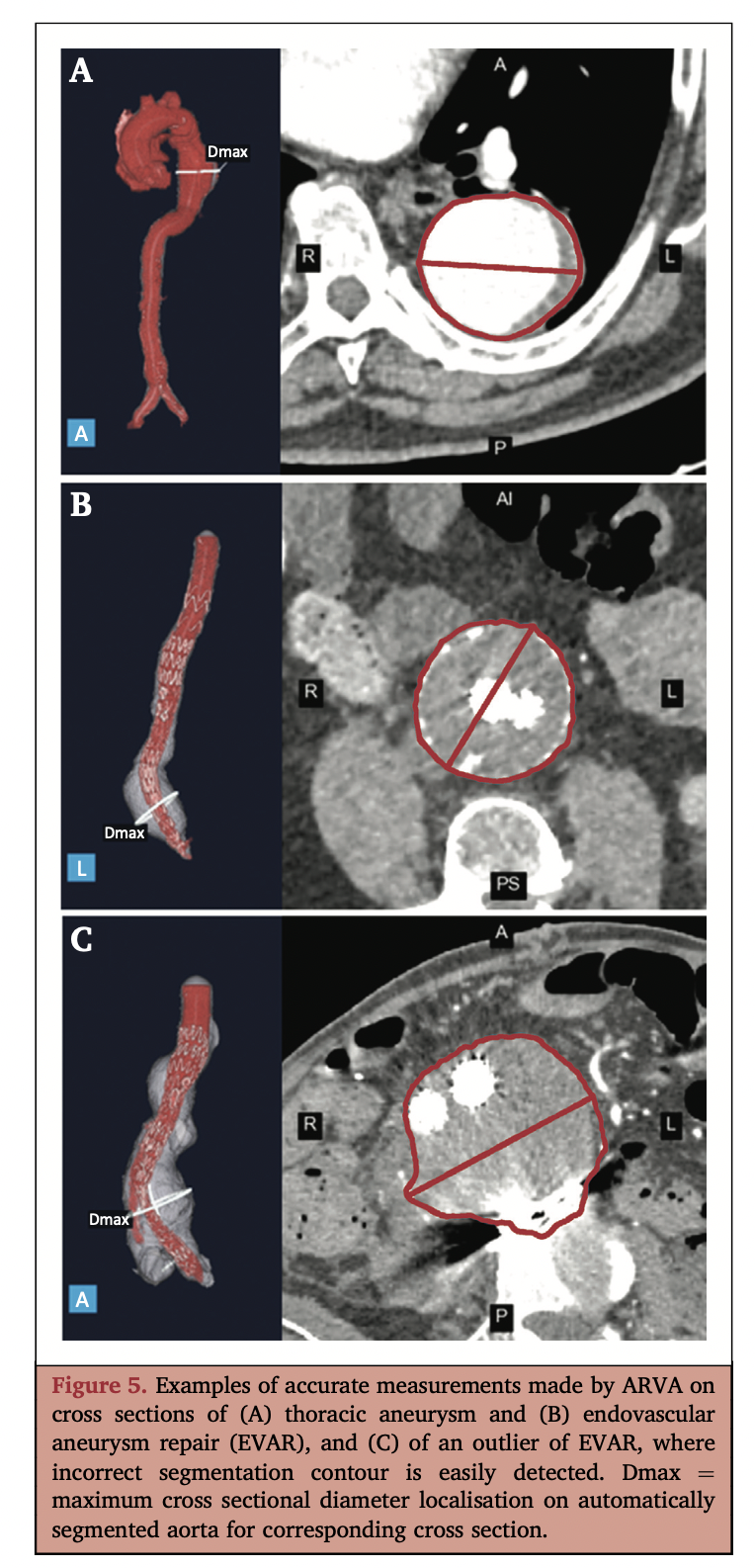
Step 5: diameter measurement. The current standard measurement in clinical practice is to measure the aortic diameter perpendicular to the centreline at the point where it is the largest. To replicate clinicians, ARVA measurements are made on the computed centreline points. For each point, the diameter of the intersection between the segmentation and the normal plane to the tangent of the centreline is measured. The maximum aortic diameter is given by the maximum of the measurements at each point. In the vicinity the iliac bifurcation, a circularity constraint is applied. If the intersection of the segmentation with the normal plane vi- olates this constraint, another point is chosen for the mea- surement following the centreline in a downward direction
Statistics
Dice score to evaluate the segmentation. A common metric used to evaluate the segmentation performance between ground truth and predicted masks is the Dice Similarity Coefficient. It is equal to twice the number of pixels in common between the ground truth mask (green) and the predicted mask (red) divided by the sum of the number of pixels in each mask (Fig. 3). Therefore, a Dice score can range between 0 (no overlap between ground truth and predicted masks) and 1 for a perfect overlap. To assess the overall segmentation performance over the entire validation set, the average Dice is reported.
While the Dice score is widely used in the data science community, it does not fully represent clinical reality as medical decisions are based on the maximum aneurysm diameter. A high Dice score does not ensure an accurate measurement. Thus, the segmentation might be precise everywhere in the aorta except in the aneurysm sac where measurements are taken. This example leads to a high Dice score but to incorrect diameters. Therefore, maximum diameter measurement error is reported.
Measurement evaluation. The absolute error between the measurements made by clinicians and the measurements made automatically by ARVA were evaluated. As the sub- sets were relatively small, the 25th, 50th, and 75th per- centiles of the absolute error distributions were recorded.
Training settings. The pipeline was implemented in Python using Keras DL library with the Tensorflow backend. Neural networks were trained on graphics processing units (NVIDIA Tesla V100) with 16 GM memory.
Nguồn: viblo.asia